
The Indian Air Force Medical Branch officially began on 13 January 1941, with the induction of its first three medical officers. For years, the story of why only three officers were selected and why this date was chosen remained an enigma. However, recently digitised documents from the National Archives of India have revealed a fascinating tale of deliberation, foresight, and practicality.
Genesis
In the formative years of the Indian Air Force, spanning from its establishment in 1933 to 1940, the medical needs of its personnel were neither independently addressed nor formally institutionalised. This was primarily due to the force’s small size and close operational integration with the RAF. At the time, IAF personnel shared airfields with the RAF, and the RAF’s Station Medical Officer provided medical cover to IAF personnel as part of the shared arrangement.
When IAF flights operated out of airfields without a stationed RAF medical officer, the nearest Army Medical Unit met their medical needs. For hospitalisation, IAF personnel were referred to British Military Hospitals (BMH) or Combined Indian Military Hospitals (CIMH).
As World War II unfolded in Europe in 1939, plans to expand the Indian Air Force were set in motion. At the time, the IAF comprised just one squadron. On 17 June 1940, the Governor-General of India approved the establishment of three IAF squadrons to be raised by 15 December 1941. These plans not only included the formation of new squadrons but also revised their establishments to include new roles.

Two of these changes were particularly notable: the role of Education Officer, previously held by an officer from the Royal Air Force, was to be Indianised, and a Flight Lieutenant from the medical branch was to be added to each squadron. This decision paved the way for the induction of three medical officers into the IAF.
The Idea: Independent Medical Service or Secondment?
Establishing medical services for the Indian Air Force was an intricate issue that required balancing operational needs with practical limitations. This responsibility fell to Group Captain J Montgomery, the Principal Medical Officer (PMO) of Air Headquarters. His initial vision was ambitious: the creation of an independent medical service specifically for the IAF. However, as the discussions progressed, it became evident that such a move would face significant challenges.
On 7 August 1940, Montgomery met with the Director General of the Indian Medical Service (I.M.S.), Lieutenant General Gordon Grey Jolly, who expressed reservations about the feasibility of establishing a separate medical branch for the IAF. The DG raised several critical points during their discussions. First, he noted that the IAF’s immediate requirement for medical officers was minimal, with only three officers needed initially to serve the planned squadrons. A cadre of just three officers would not justify the administrative and logistical efforts required to establish a new, standalone medical service.
The second challenge was related to career progression. Unlike the I.M.S., which offered permanent appointments and a structured path for advancement, the proposed IAF medical service would not provide similar opportunities. Officers assigned to such a small cadre would find themselves in a professional dead-end, unable to achieve the career growth the I.M.S. could offer. This lack of long-term prospects could deter talented and qualified medical professionals from joining the IAF.
Additionally, the DG pointed out the inherent vulnerabilities of a small cadre. With just three officers, the branch would be perpetually at risk of disruptions due to leave, resignations, or casualties.
The final issue revolved around resource allocation. The I.M.S. was already responsible for supplying medical officers to various departments, including military, civil, research, Burma, E.A.&P. Department, and Port Health Medical Services. Dedicating resources exclusively to the IAF when the demand was so limited could strain the I.M.S. and disrupt its ability to fulfil its other commitments. As a result, the D.G. proposed a more pragmatic alternative: the secondment of I.M.S. officers to the IAF on fixed-term appointments.
Montgomery initially expressed disappointment at abandoning the idea of an independent medical branch. However, he recognised the merit of the DG’s arguments. He agreed that the secondment of officers from the I.M.S. would address the IAF’s immediate needs without overburdening existing structures. At the same time, he insisted that the door should remain open to create a dedicated IAF medical branch in the future, particularly if the branch’s requirements grew significantly during the war.
By the end of these discussions, it was clear that secondment was the most practical solution for meeting the IAF’s immediate needs. The arrangement offered flexibility while preserving the possibility of establishing a standalone medical branch in the future, should the extent of the IAF’s operations warrant such a move.
The Curated Ask
The secondment of I.M.S. officers to the Indian Air Force was formalised in the Air Force Instructions (India) on 23 November 1940.
Specific eligibility criteria were outlined to ensure that the officers seconded to the IAF could meet the unique challenges of aviation medicine. Candidates had to be under 32 years of age and possess 1–3 years of service in the I.M.S., striking a balance between youth and experience. Preference was given to officers with degrees from British universities or experience in aviation-relevant fields, such as hygiene, eye testing, and psychological assessments.
The responsibilities of I.M.S. officers in the IAF extended beyond conventional medical duties. They were tasked with detecting and managing the physical and psychological challenges unique to flying. This included monitoring aircrew for early signs of flying stress, anxiety, neurosis, and other psychological manifestations.
The officers were expected to cultivate strong relationships with the aircrew, as trust and camaraderie were essential for identifying and addressing medical or psychological issues. They were also required to accompany flights as passengers when necessary, allowing them to observe the operational environment firsthand and better understand the challenges faced by aircrew.
Montgomery and the DG devised a straightforward process to ensure the secondment arrangement’s success. The I.M.S. would handle the recruitment of officers, calling for volunteers from within its ranks who were interested in serving with the IAF. Once applications were received, Air Headquarters would conduct interviews to select officers who met the IAF’s specific needs.
Montgomery also emphasised that the arrangement should foster a sense of belonging among seconded officers. He suggested integrating them into the IAF’s organisational structure. Officers retained their original I.M.S. ranks—Lieutenant, Captain, and Major—but were assigned equivalent IAF ranks of Flying Officer, Flight Lieutenant, and Squadron Leader.
The secondment framework ensured that officers retained their I.M.S. pay scales and continued to accrue benefits, such as pensions and gratuities as if they had remained in the I.M.S. They were also eligible for additional allowances for flying duties while serving with the IAF. Seconded officers wore their I.M.S. service dress during their tenure in the IAF.
Seconded officers initially served a one-year probationary period, during which their performance was closely monitored. If they proved suitable, their service could be extended for the duration of the war. These measures were intended to ensure the commitment and morale of seconded officers, enabling them to perform their duties effectively.
The Selection
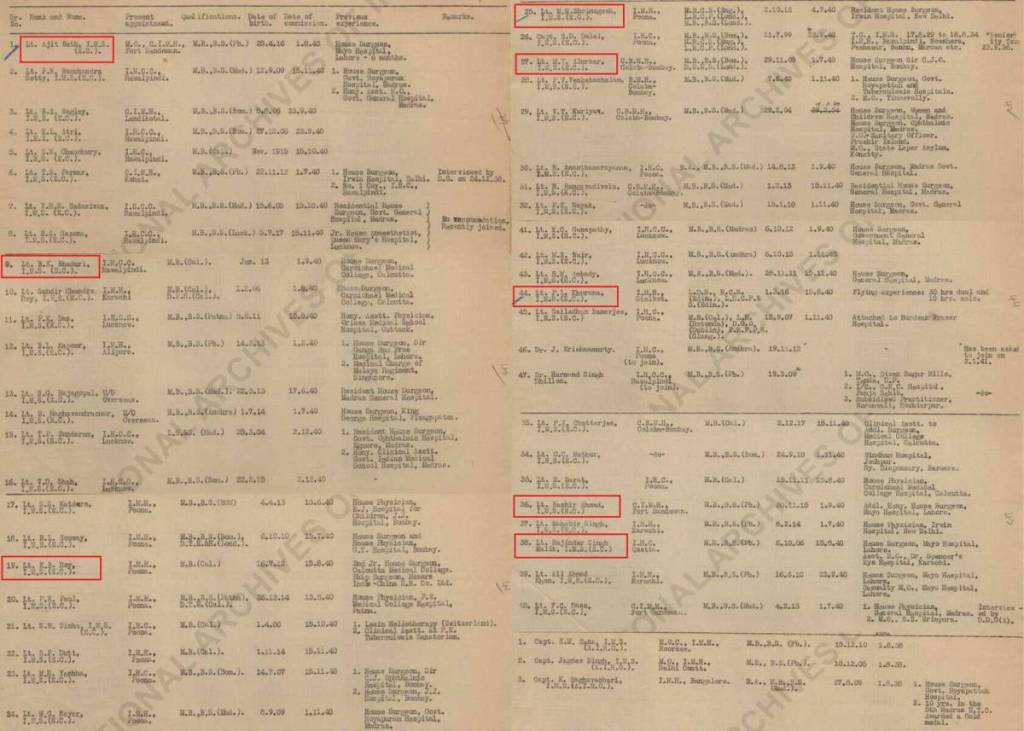
Once applications were received, they were reviewed by the I.M.S. and Air Headquarters. The result was a shortlist of 50 candidates (366 IMS officers in total in India) who met the eligibility, competency and recommendation criteria. This list was sent to Group Captain T.C. Montgomery for further scrutiny, who was entrusted with selecting the final three officers from this pool—a task that demanded careful deliberation given the strategic importance of this first group.
Montgomery used a combination of professional qualifications, field experience, and personal attributes to make his selections. Montgomery placed special emphasis on officers who had experience working in challenging environments, such as remote military hospitals, where resourcefulness and resilience were critical. He also valued candidates with a track record of building strong relationships with their colleagues, a quality essential for fostering trust with aircrew. Officers with prior exposure to flying or aviation medicine were given additional weight, as this experience was considered invaluable for understanding the unique demands of serving in an Air Force setting.
After a thorough evaluation, three officers were chosen:
- Lieutenant Ajit Nath: Serving as the Medical Officer at Fort Sandeman, Ajit Nath brought experience as a surgeon, having previously worked at the prestigious Mayo Hospital in Lahore.
- Lieutenant M.M. Shrinagesh: Posted at the Military Hospital in Poona, Shrinagesh had a distinguished record as a resident surgeon at Irwin Hospital in Delhi.
- Lieutenant P.L. Khurana: Stationed at the Military Hospital in Sialkot, Khurana was unique among the candidates, as he was the only one with prior flying experience. He had logged 30 dual and 10 solo hours in civil aviation, an asset Montgomery believed would give him a distinct edge in understanding the medical needs of aircrew.

Interestingly, many of the officers from the original list of 50 were later seconded to the IAF as the demand for medical personnel grew during World War II. In fact, the first ten officers came from the initial list. The selection process succeeded in not only identifying the first three officers but also creating a pipeline of qualified and enthusiastic candidates for future requirements.
On 24 December 1940, Air Headquarters issued formal orders confirming the selection of the three officers. They were instructed to report to the IAF Medical Board in Lahore on 13 January 1941 for a short training course on Air Force organisation and medical routines.

The Beginning
The three newly selected medical officers of the Indian Air Force—now holding the IAF rank of Flying Officer—Ajit Nath, M.M. Shrinagesh, and P.L. Khurana—reported to Lahore on 13 January 1941, marking the official birth of the IAF Medical Branch. This date, immortalised in IAF history, symbolises the beginning of a critical support structure for the Air Force.
Upon their arrival in Lahore, the three officers underwent a brief training program at the IAF Medical Board. After completing their training, the three officers were assigned to key IAF bases on 23 January 1941:
- Ajit Nath was posted to the Initial Training College at Lahore, one of the central hubs for training Air Force personnel.
- M.M. Shrinagesh was assigned to Station Headquarters Ambala, one of northern India’s busiest and most strategically significant air bases.
- P.L. Khurana was posted to the Aircraft Depot in Lahore, which served as a critical logistics and maintenance hub for the IAF/ RAF.
On 1 April 1941, Ajit Nath became the first medical officer of No. 1 Squadron, the oldest unit in the Indian Air Force. Soon after, MM Shrinagesh and P.L. Khurana followed, taking up similar roles in other squadrons.

As World War II escalated, the demand for medical officers in the IAF surged. The initial plan to appoint only three officers quickly proved insufficient, prompting Air Headquarters to revisit the initial selection pool of 50 shortlisted candidates. Many of these candidates were seconded to the IAF over the subsequent months and years, supporting the rapid expansion of the Medical Branch to meet operational demands.
In May 1941, Harjinder Singh Malik joined the IAF as the fourth medical officer. By the end of 1941, three more officers—M.Y. Alurkar, B.K. Bhadury and N.N. Dutt were inducted into the medical branch, and all of them were part of the original shortlist. Notably, P.L. Khurana continued to make his mark by becoming the first medical officer permitted to undertake flying duties. However, his flying career faced a setback when he was involved in an accident at Ambala during a sortie in a Hurricane.

The IAF Medical Branch, which began modestly, steadily gained momentum. According to the Bharat Rakshak Database, 2,735 medical officers have been commissioned in the IAF since 13 January 1941.
⭐ This post previously received 5.0/5 from 75 readers in our legacy system.




Leave a Reply